This is a post from Francis Collins, the Director of the National Institutes of Health, and a well-known geneticist. It explains how genome sequencing can help people with a rare and unexplained genetic disease. I think he explains it clearly, what do you think? Is there anything that’s too technical for the layperson?
Archives for category: Uncategorized
In the summer of 2012-13 my daughter Katherine and her friends got together to make a short film during their holidays while they waited for their University offers.
Nearly two years later here it is.


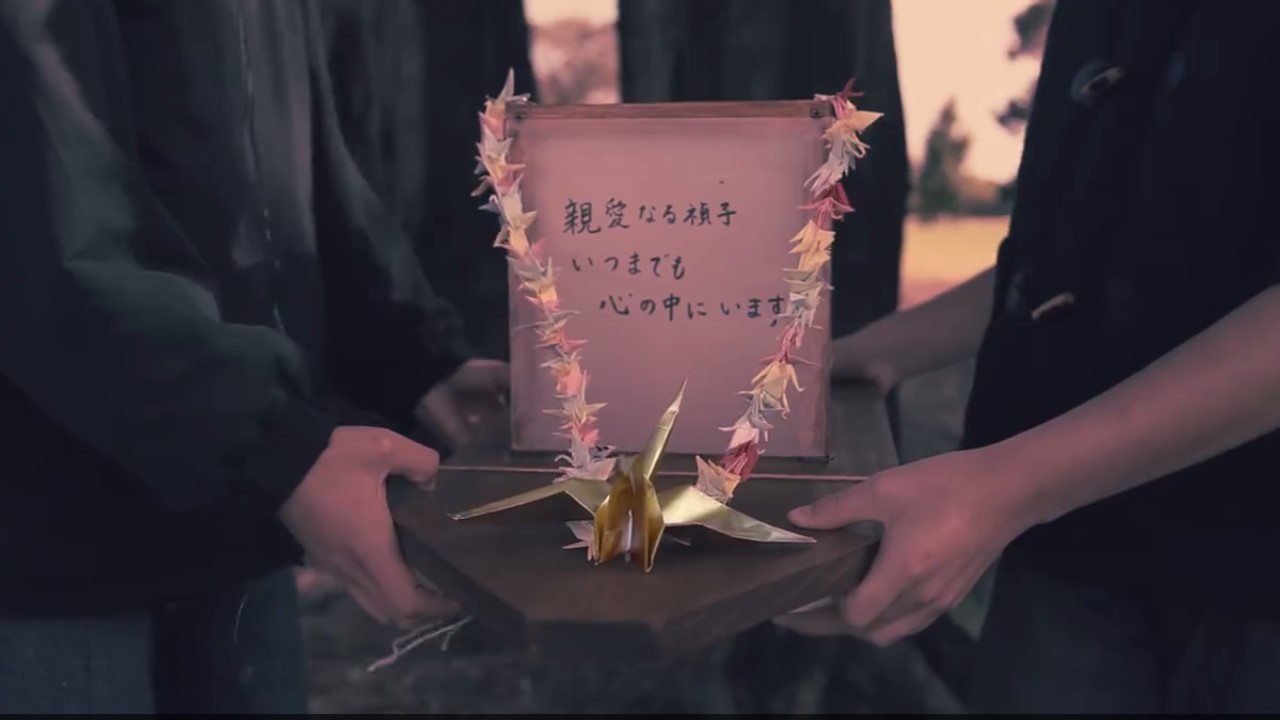
Paper Thin is based on the true story of Sadako Sasaki, who tried to fold 1,000 paper cranes to beat her leukaemia. This is an amazing short film directed by Elizabeth Duong with beautiful original music by Daniel Hernandez and Elle Graham. Don’t just take my word for it. Don’t just watch it. Don’t just like it.
Share Paper Thin to help make leukaemia HISTORY.
A generous, dedicated group of people have been working hard to create the story of Sadako Sasaki in film to support our leukaemia research project.
Sadako survived the Hiroshima bombing in 1945. Radiation can kill quickly by causing radiation sickness, or slowly by causing cancer. Like many other children who survived the bomb, Sadako developed leukaemia ten years later when she was 12.

The Director Elizabeth Duong and the Paper Thin Productions team is poweful both visually and emotionally. Daniel Hernandez and Elle Graham’s music can stand on its own.
So why Paper Thin? The story ties in with our research into leukaemia, and we’re aiming to raise awareness and support for the research.
This is crowdsourcing with a difference. Researchers worldwide are looking to alternative sources of funding as grant funding gets more and more competitive. Missing out on grant funding is not a short term problem. One very real problem is that skilled Scientists have to leave research. That means the projects they’re working on stop and discoveries they were after will never happen. The expertise they’ve build up won’t be used.
The most risky projects are the ones that make the biggest difference, the game-changing discoveries. But granting bodies don’t like risky projects. They like giving money to the big labs – this means more of the same.
Crowdsourcing is gaining in popularity – the people decide for themselves what research projects their donations will help. In the case if Paper Thin there’s no middle-man crowdsourcing platform (they take a commission).
Another big difference is the product – this is a leukaemia story in film and music.
So because the Paper Thin Productions team’s given their time freely you can be sure 100% of your donation will go to the research.
THANK-YOU TO ALL INVOLVED
The credits do better justice than I could to acknowledge the people who helped. Special thanks also to Jenny Going from the Essendon Symphony Orchestra for allowing us to use their time to rehearse and record the music, and also to Shauna Hurley, Bridget Bible, Richard Prentice, Barabara Cytowicz, Leslea Johnson, Amber Atkinson and Kayanne Allan from St Vincent’s Hospital who helped with the logistics of how to do this from the Hospital’s perspective.
I was privileged to speak at the Aspiring Women in Science conference in Brisbane, Australia last month. I think this is a fantastic initiative, which gives senior school girls an insight into working in various fields of Science (including Engineering and Medical specialties). Girls from years 10, 11 and 12 from all over Queensland were invited (mostly aged 15-17). Why girls? I attended a few of the talks myself and it reinforced my own view that there are experiences and conditions specific to women in Science. In talks on Science-as-a-career, information and advice from a woman’s perspective wouldn’t normally come up. It’s only fair to be as informed as possible when making a life choice. Both research and non-research careers were featured in the conference program.
We heard a lot of inspirational stories from Scientists in many different fields. Professor Ian Frazer – inventor of the Human Papilloma Virus vaccine Gardasil – was the keynote speaker. He spoke of his exciting adventures of discovery, from his childhood in Scotland to fulfilling his dream of building the Translational Research Institute in Brisbane. His dream will allow local scientific discoveries to be developed to commercialisation in Australia, instead of being sold to overseas companies. The virus (HPV) is a major cause of female cancer deaths in developing countries, and Prof Frazer is still battling to spread this message.
In the other sessions many women spoke of their work, of what excites and challenges all Scientists, and the challenges that women in Science in face because they’re women. Although we like to think that parents have equal roles nowadays, a woman in research will likely have to decide whether she puts her children in childcare from a young age or give up research. Grandparents and other extended family are often not around to help because research fields are so specialised that researchers are likely to live far from their home town. These are stories that are familiar to me and were reinforced as I spoke to and listened to other women.
Several researchers, including Prof Frazer, spoke of the frustration of grant writing, the pressure of finding research funds, and the difficulty of sustaining a research career through short-term employment cycles. But more than one researcher also mentioned a published research study showing that a female name on an application for a (US) University Science position means the applicant is less likely to win the job, and the starting salary will probably be lower. Women also compete for grants, publication, promotion and leadership roles. And they drop out faster than men.
I don’t want to sound too negative, but students should be informed when they’re planning their future. I also believe things are slowly improving and if we keep on challenging the system it will keep on getting better. Being aware of the problem is part of working for a solution.
I can speak for scientific research and the thrill of discovery – if it excites you and you’re willing to give it a go – then go for it. Determination is part of the secret of success. I’m inspired by Jim Carrey’s lesson from his father: “You can fail at what you don’t want, so you might as well take a chance on doing what you love.”
But I do think that if you’re taking a risk it will be a bolder and better one if you have a safety net – such as family support, or a professional qualification as a backup plan.
I can’t pass up the opportunity to present these words from one inspirational woman about another, Maya Angelou (nothing to do with Science).
The Aspiring Women in Science conference was co-ordinated by Ela Martin and St Aidan’s Anglican Girls’ School in Brisbane. Part of the reason I was invited to speak is my history as a past student. I admire the school for making this conference and the school’s facilities and resources available to ALL girls in Queensland. Queensland’s a big place and some girls travelled a long way to make it. So, to Ela Martin and St Aidan’s, to Queensland University who supported the conference, and to all the Scientists who gave their time, a big thank-you for your initiative. I hope this idea has wings – per volar sunata.
(This is cross-posted from the Fireside Science blog at SciFund Challenge.)
We care about our health and the health of our loved ones. If only we had explanations and cures for all of humanity’s illnesses. But there are still many diseases that aren’t being researched, even though they cause real and obvious suffering.
Medical research is paid for in a number of ways. The obvious one is the drug companies, where there’s a cost-benefit consideration. I’ll discuss the other options, and how it works in Australia.
The biggest pool of money comes from the government. We have the National Health and Medical Research Council (NHMRC), which runs several grant funding schemes each year. There are also some Fellowships that provide researchers with a secure salary for up to five years. Research grants typically last three years, and they usually include salaries for scientists working on the project. Only 16.9% of Project Grant applications were funded for this year. And the competition gets stiffer every year. So this is clearly not a reliable source of funding for most research wish lists. In the words of the crowdfunding site microryza, “Our system for funding science is broken. Our planet’s biggest funders are so conservative that they fund … only the most obvious ideas. Discoveries that matter are languishing.”
Charitable giving picks up a lot of research that the government doesn’t fund. Besides the work they do supporting patients and their families, some patient advocate groups raise funds for research. There are also private citizens who set up research trusts, and many many more who donate to research. Most of these charities and trusts pull less weight than the government grants, but there are some very large ones based overseas, such as the Wellcome Trust and the Bill & Melinda Gates Foundation.
There’s also a new movement known as crowdfunding. You may have heard of Kickstarter. There are other crowdfunding sites specifically for scientific research. Examples are microryza (now renamed experiment), Petridish, and SciFund Challenge. There have been some remarkable successes like the microbiome project but most projects ask for a modest amount. Researchers are turning to crowdfunding more and more as other sources of funding become harder to get.
So there’s a limited pot of money for research. Who decides what it’s used for? Government grants are hotly contested. One of the tasks of the grant writer is to convince the reviewers that theirs is an important problem and the team has the expertise to solve it. Some charitable trusts have a similar review system, but it can also vary quite a lot and can depend on the wishes of the donors. Crowdfunding cuts out the middle man and it’s the donor who must be convinced that the project is worthwhile.
So, why isn’t there more research into your disease and what can you do about it?
You will need researchers who have an interest in your disease and some funding. Which brings us to awareness. Greater awareness by governments, policy makers, researchers, and doctors who make diagnoses will help your case. Under-recognition of rare diseases is a huge problem which can also be addressed by awareness.
The common and high profile diseases such as cancer get a lot of research dollars. Their severity and impact on the community are obvious. Rare diseases don’t have this advantage. Rare Disease Day is an annual event that advocates for people with diseases, syndromes and conditions that occur in fewer than one in 2,000 people. Rare Disease Day is coming up – most years it falls on the 28th February, but every fourth year or 1,461st day it falls on that rare date – 29th February.
Patient advocate groups that offer research grants can have some influence. They can offer grants that are targeted to a specific disease or question. This can help them find researchers with the appropriate expertise, and attract researchers who are looking for funding. They can use the funds that have been raised specifically to improve the lives of the people they support. Crowdfunding is also a great way to target donors who are keen to support the cause.
About 80% of rare diseases are caused by genetic errors. Humans have over 3,000,000,000 letters in their genetic makeup, and these spell out over 20,000 pairs of genes. Many genetic diseases are caused by a one letter error in one of these genes. The human DNA sequence is now mostly known, so it’s possible to read the DNA sequence of the patient and compare it to a standard to find a needle-in-a-haystack DNA error. Unfortunately not all genetic diseases are that straightforward – but it’s a start.
Recently there have been some heart-warming examples of very rare but debilitating diseases for which the causes have been found with the help of sequencing and a persistent parent, being in the right place at the right time, or scientists who were looking for a problem to solve. These are some of the good news stories of modern genetics that are starting to make an impact on rare diseases.
If you want to help make a difference my advice is to support your disease’s patient advocate group, fundraise and lobby for research. If there isn’t a support group for your disease, you could start one. If your disease is rare, Rare Disease Day is there to help. And anyone can help raise awareness about a disease. Better awareness brings better understanding.
LINKS TO PERSONAL GENOME STORIES
Cracking the code – transcript of the Australian Story episode on ABC TV. A father’s quest to find the gene mutation causing his son’s disease.
Genome maps solve medical mystery for Calif. twins – Shots – Health news from NPR.
“We gained hope.” The story of Lilly Grossman’s genome – National Geographic’s Phenomena – Not Exactly Rocket Science
James Lupski’s Research into His Disease Paved Way Toward Personalized Medicine – Quest (MDA Magazine Online – Fighting Muscle Disease)
The Solution to Diagnostic Delay May Be Closer Than We Think – blog post by the National Organization for Rare Disorders arguing that a rare disease app may help doctors diagnose rare diseases: “…most… rare diseases are unfamiliar to doctors… When doctors are unable to explain patients’ symptoms — as they are for at least three years in the majority of rare disease cases — psychiatric diagnosis is made by default.”
Chromosomes that cause cancer: Chromosomes with two centromeres and the breakage-fusion-bridge cycle
Barbara McClintock published a paper describing the breakage-fusion-bridge (BFB) cycle in 1939. Many of her ideas were well before their time. Like many such profound leaps in thinking, the BFB cycle took a long time to catch on. She wrote in 1973, “I stopped publishing detailed reports long ago when I realized, and acutely, the extent of disinterest and lack of confidence in the conclusions I was drawing …One must await the right time for conceptual change.” Her work was appreciated much later and she was awarded a Nobel Prize in 1983 for her discovery of “jumping genes“.
A few weeks back I introduced this post by describing normal chromosome division. This time we’ll look at the breakage-fusion-bridge cycle. This is one way chromosome division can go wrong. Very wrong, in the sense that it can cause the chromosomes to keep changing, and this can cause cancer.
A human chromosome with two centromeres is abnormal. Chromosomes with two centromeres are not unusual in cancer cells. In fact they’re probably a lot more common than we think, because in both research and diagnostic labs the centromeres are usually not looked at.
To recap, a normal chromosome has one centromere. Before the chromosome divides, the two identical halves (chromatids) are held together at the centromere. When the chromosome divides the centromere splits into two halves, the chromatids become the new chromosomes, and the centromeres take the two new chromosomes in different directions into the two new daughter cells.
So what happens if there are two centromeres? If they’re both aligned so that they head in the same direction it’s not a problem – together they take a complete new chromosome with them. The closer the centromeres are together the more likely this is.
Now follow the pictures and their captions. These describe chromosome division in an abnormal chromosome with two centromeres. Especially follow the yellow dots.

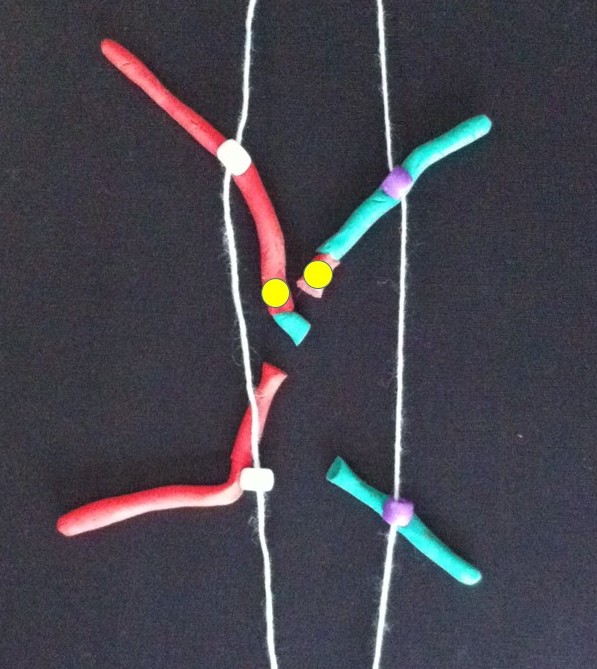
If the two centromeres on a chromosome go in the same direction there’s no problem. But if there’s a twist between the two centromeres when the chromosomes align ready for chromosome division….

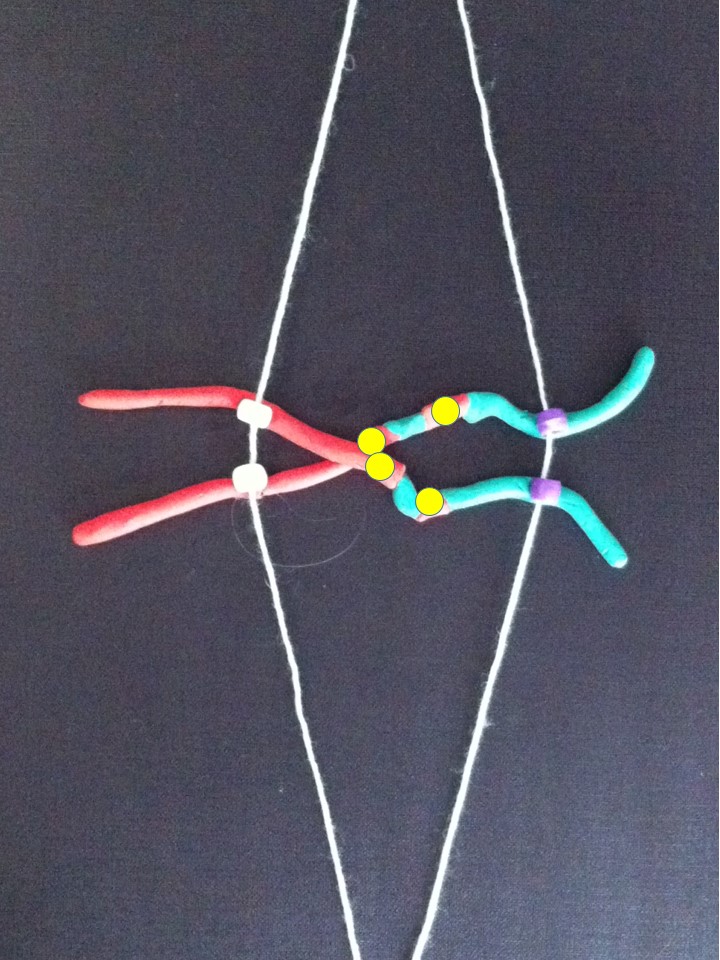
….then, when the two halves of each centromere separate they go in opposite directions. We have a “bridge” spanning the gap between the two centromeres.
The bridge is stretched and can break.

The broken chromosomes in the new cell join together – the top daughter cell gets an extra copy of the yellow gene. The bottom cell loses this copy of the yellow gene.

The new chromosome copies itself to make two equal halves.
If this process repeats..

…

Fusion of the broken pieces creates a chromosome with four copies of the yellow gene.

After replication.
If the yellow gene in the pictures is a cancer gene (“oncogene”) the cell with extra copies might grow and multiply faster than its neighbours. We call this natural selection – the cells that can grow faster than their neighbours become more common which means the genetic change causing that is undergoing “positive selection”. Yes, the cells in our body can evolve and we know this best as cancer.
All this change happens between the two centromeres where the bridge forms. So if we find a chromosome with this type of change on one side of the centromere only it’s a clue that this might have been caused by the breakage-fusion-bridge cycle.
These are modelling clay images from my breakage-fusion-bridge claymation. They’re a bit rough but I hope it helps you understand what happens. Many, perhaps most, images demonstrating the BFB cycle show a different version – where the abnormal chromosome is created by two chromatids of one chromosome breaking and joining together. Most examples don’t show the version I’ve presented – where two different chromosomes have joined together. Check this out on Google Images (search for breakage-fusion-bridge).
Here’s the answer to the quiz from the telomere post. The arrows point to the ring chromosomes. Being rings they have no ends, so no telomeres.

Further Reading:
B. McClintock 1939. The Behavior in Successive Nuclear Divisions of a Chromosome Broken at Meiosis. Proc Natl Acad Sci U S A. 1939 August; 25(8): 405–416.
M. Kinsella and V. Bafna 2012. Combinatorics of the Breakage-Fusion-Bridge Mechanism. J Comput Biol. 2012 June; 19(6): 662–678.
R. MacKinnon and L. Campbell 2011. The Role of Dicentric Chromosome Formation and Secondary Centromere Deletion in the Evolution of Myeloid Malignancy. Genetics Research InternationalVolume 2011 (2011), Article ID 643628.
Related articles
- What is a Centromere and How Does it Contribute to Mitosis? (biology.answers.com)
- Understanding the Anatomy of Sister Chromatids (biology.answers.com)
The new Fireside Science blog at SciFund Challenge
I know, it’s been a long time between posts. I’m working on a breakage-fusion-bridge claymation to show how some cancer chromosomes are very changeable. It’s a steep learning curve but hopefully I’ll have it thoroughly mastered soon.
In the meantime here’s a post from Abby Buchwalter in the new group blog “Fireside Science” – SciFund Challenge’s Guide to Life, the Universe, and Everything. Abby and some of the other graduates of the first SciFund Challenge course (including myself) have started a group blog hosted by the SciFund Challenge website. Here we plan to bring the world of Science to readers in an easily digested form.
Abby describes a cell using only the 1,000 most common words in the English language.
Enjoy.
Related articles
- The new Fireside Science blog at SciFund Challenge (chromosomesandcancer.com)
- Fireside Science (scifundchallenge.org)
- A diagram of a cell, “Up-Goer Five” style (scifundchallenge.org)
