Susan Sontag survived uterine and breast cancer, but as sometimes happens, the treatment that cured her eventually caused the MDS that killed her (“therapy-related MDS” or t-MDS). Her son David Rieff gives some insight into her illness in his bookSwimming in a Sea of Death: A Son’s Memoir (Granta). After a bone marrow transplant, her disease became full-blown leukaemia. (Not all cases of MDS are this severe.)
Chromosome analysis of the MDS cells is one of the tests used to predict the patient’s outlook. “The spectacularly difficult cytogenetics of her specific case” (very abnormal chromosomes), as Rieff puts it, means she had a poor chance of survival.
Sontag stands out as a patient because she wrote about illness, in her philosophical book Illness as Metaphor. I came across the story of her treatment and one of her quotes about illness in Siddhartha Mukherjee’s very readable book, The Emperor of All Maladies: A Biography of Cancer.
“Illness is the night-side of life, a more onerous citizenship. Everyone who is born holds dual citizenship, in the kingdom of the well, and in the kingdom of the sick. Although we all prefer to use only the good passport, sooner or later each of us is obliged, at least for a spell, to identify ourselves as citizens of that other place.”
Susan Sontag, Illness as Metaphor. Published by Farrar, Straus and Giroux (1978)
25th October is World MDS Awareness Day. This article is part of a series about high-profile MDS patients.
In the summer of 2012-13 my daughter Katherine and her friends got together to make a short film during their holidays while they waited for their University offers.
Paper Thin is based on the true story of Sadako Sasaki, who tried to fold 1,000 paper cranes to beat her leukaemia. This is an amazing short film directed by Elizabeth Duong with beautiful original music by Daniel Hernandez and Elle Graham. Don’t just take my word for it. Don’t just watch it. Don’t just like it.
Carl Sagan was an astronomer and academic, best known for popularising astronomy. He hosted and co-produced the original hugely popular series Cosmos: A Personal Voyage. Its sequel Cosmos: A Spacetime Odyssey was released this year. Even though I’m a biologist at heart I was fascinated by the original Cosmos.
Sagan was diagnosed with a myelodysplastic syndrome (MDS) and died at the age of 62, in 1996. In interviews near the end of his life he discussed myelodysplasia and said he was hopeful he’d been cured. He died at the Fred Hutchinson Cancer Research Center of pneumonia after his third bone marrow transplant, a complication of this illness.
Most people with a diagnosis of MDS won’t have heard of it before. MDS is a group of bone marrow diseases. It’s at least as common as or more common than leukaemia but older people have a higher risk – perhaps one in 2,000 over the age of 60. A third of people with MDS will develop leukaemia. The 14th July, 2014, is the Leukaemia Foundation of Australia‘s second National MDS Day . One of the aims of MDS Day is to raise awareness of MDS.
Sagan’s illness was an opportunity to popularise MDS, but look how the cause of his death was described in these TV news reports.
In these news stories he was said to have died from a complication of “a rare blood disorder that led to cancer”, or “a blood disease”, “a bone marrow disease”, and even a” bone cancer” – the name of his disease was avoided.
Myelodysplasia literally means abnormal bone marrow cells. Blood cells are made in the bone marrow. In MDS the immature bone marow cells are abnormal and don’t mature properly. So the blood doesn’t have enough normal blood cells to do its job effectively. The blood is made of a number of different types of cells and the different types of MDS relate to the type of abnormal cell. MDS is often associated with a recognised chromosome abnormality, and identifying these chromosome abnormalities can help with diagnosis, treatment and prognosis. Therapy-related MDS is a specific type of MDS caused by treatment for a previous unrelated cancer and it usually has a poor outcome and very abnormal chromosomes.
MDS research has been neglected but has picked up recently. Some of the recent progress includes work by Carl Walkley and Louise Purton at St Vincent’s Institute in Melbourne, Australia.
MDS has had a history of name changes that seems to have made the meaning of its name less clear, except to medically trained people. This hasn’t helped improve public awareness of MDS. It was first named Di Guglielmo Syndrome in 1923 after its discoverer, then became refractory anaemia, then preleukaemic anaemia, preleukaemic acute human leukaemia, preleukaemia, and finally in 1976 the French-American-British Co-Operative Group of haematologists named it myelodysplastic syndromes. This recognised that it’s a group of related diseases and that not all cases will go on to develop into leukaemia.
Pathologist Ed Uthman, thinks Sagan’s Disease would be a better name for myelodysplastic syndromes – both as a tribute to Carl Sagan and a name that would mean more to most people than myelodysplastic syndromes. Maybe he has something. Plenty of syndromes and diseases are named after people who studied them. Down Syndrome would have to be the best known example. Have you heard of amyotrophic lateral sclerosis? Motor neurone disease? Lou Gehrig’s disease? The first name is probably a nice technical description of the disease, but I’m guessing you’re more likely to have an idea of what the disease is from one of the last two names, because they’re used in popular media and are connected in the public eye with famous sufferers – Stephen Hawking and Lou Gehrig. (Ed Uthman also think’s Lou Gehrig’s Disease should be “Hawking’s Disease”.)
I’ll let Carl Sagan have the last words on popular (mis)understanding of science (extract from Wikiquote).
We live in a society absolutely dependent on science and technology and yet have cleverly arranged things so that almost no one understands science and technology. That’s a clear prescription for disaster.
Every kid starts out as a natural-born scientist, and then we beat it out of them. A few trickle through the system with their wonder and enthusiasm for science intact.
This is the opening title of Paper Thin. Yesterday was the last day of filming and I got a look at some of the Director/Producer Elizabeth Duong‘s work. It’s exciting – this will be a touching but beautiful film. It’s based on a true story of a girl called Sadako who developed leukaemia after exposure to radiation in Hiroshima.
One of the hallmarks of leukaemia that’s caused by radiation or toxic chemicals is very rearranged chromosomes. I’m working on unravelling the patterns and causes of the very disorganised genetics of this type of leukaemia (known as therapy-related acute myeloid leukaemia).
Sadako hoped for a cure. My hope is that with the help of this film this research can continue and realise her dream for future leukaemia patients. A big thank-you to Elizabeth and all her helpers, who have given their time freely. A special mention also to Daniel Hernandez who composed the original soundtrack. It’s awesome. Here we have Essendon Symphony playing the opening theme and I think that’s Daniel playing over the stings.
Cancer has been described as the most common genetic disease. This doesn’t necessarily mean it’s hereditary – usually the genetic mistakes that cause cancer arise in the body’s organs or tissues and can’t be inherited. We’re continually learning of new cancer-causing genetic mistakes.
If we think of genes as words spelling out the instructions for our bodies to function, there are different types of mistakes or “typos” that can cause cancer. Some of these are like spelling mistakes – an incorrect letter or two. The mistakes I’ll be talking about here involve whole words (or lots of them). For example one or more copies of a word are added – ” very big” becomes “very very big” – extra copies of a cancer gene (we call them oncogenes) can cause or accelerate cancer growth. Or if a word is lost – “don’t grow” becomes “grow” – this illustrates loss of a tumour suppressor gene.
I described the breakage-fusion-bridge cycle a few weeks back. The BFB cycle was a theory developed from studies with maize, but it also applies to some cancers. This is an example of basic research, inspired by curiosity but eventually being useful in ways we never imagined. If you look back at that post it shows how the BFB cycle can cause gain or loss of genes. If a cancer gene is multiplied, or if a tumour suppressor gene is in the part that’s lost, the cell can gain a growth advantage over other cells, which is part of the process causing cancer.
Here’s an example.
Cancer cell lines are cancer cells that can be grown indefinitely in the laboratory. I’ve just published a paper on HEL, which is a leukaemia cell line. It’s popular for studying how cells make globin (molecules in red blood cells that help us process the air we breathe).
One of the gene abnormalities in HEL is amplification of the JAK2 gene. JAK2 is a well-known cancer gene that is often abnormal in blood cancers. The normal gene can be mutated to become a cancer gene, for example by a “spelling mistake” in the DNA. By adding extra copies of this abnormal gene the effects can be magnified. This is known as gene amplification. There are a few cancer genes that are commonly amplified in cancers.
To cut a long story short, JAK2 is amplified in the HEL cell line. And a nearby tumour suppressor gene (CDKN2A) has been lost. But only by looking at the chromosomes does the reason become clear. Some detective work tells us that there were some breakage-fusion-bridge events. I won’t go into the detail – if you’re interested it’s in the paper. But we have chromosomes whose ancestors had two centromeres, and if we use a DNA tag for the region between the centromeres we can see “stripes”.
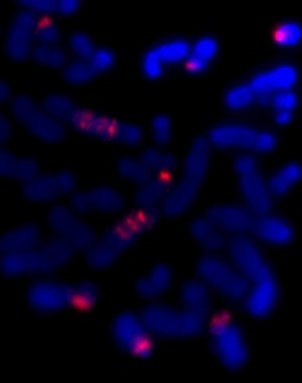
Here’s an example from HEL that shows DNA amplified by the BFB cycle – we can show where a gene is on the chromosomes by labelling it with a fluorescence tagged DNA “probe”. The striped pattern reminds us of the yellow dots in the modelling clay demonstration:
The red is DNA that’s normally at one end of some of the chromosomes. The stripes tell us that the end of a chromosome (22) is in the middle of these chromosomes and there are extra copies. It’s a strong clue that BFB cycles were involved and the ancestral chromosome had two centromeres.
The new chromosome with four copies of the yellow gene courtesy of the breakage-fusion-bridge cycle.
Recently JAK2 amplification was also reported in triple-negative breast cancer. Triple negative means that three well-known genetic causes of breast cancer are not present. So finding JAK2 amplification would help explain the cause of some triple-negative breast cancers, and could help work out an effective treatment. Perhaps this JAK2 amplification is sometimes caused by BFB cycles. Without looking at the layout of the abnormal chromosomes we may never know.
Getting back to Paper Thin. I’ve been privileged to have a bit of insight into the filming process recently.
Elizabeth Duong and her team of volunteers are producing a short film to raise awareness of leukaemia and, fingers crossed, some research funds. I’m amazed at how professional this amateur film-maker is.
Elizabeth at work with the lead actor.
We were fortunate to get the use of a hospital bed for filming, thanks to Kayanne and Amber at St Vincent’s Hospital. So just by being there at the start and end of filming days, and helping set up for the final day, I feel like I know a bit more about it all. We’ve also had a loan of original 1950s props from the St Vincent’s Archives (courtesy of the archivist, Barbara).
Costumes by Estelle
And lots of people were roped in to help make paper cranes – the target was 1,000 but I think there were multiples of that in the end.
Here are some shots from set-up. Elizabeth and Katherine were stringing paper cranes up around the bed late into the night. Everyone’s been making the most of Uni holidays to get stuck into the film.
When it was initiated by the US Department of Energy in 1987, the Human Genome Project was an ambitious, some said impossible, endeavour. It was all about producing a representative readout of the human genome – that is, the whole set of human DNA.
At the time DNA was read (sequenced) manually – scientists read each letter of the code off an X-ray film. One by one genes were laboriously found and sequenced. Finding and characterising a gene in this way was a whole PhD project, if you got lucky and actually found the gene (finding a gene by family studies was harder than starting with a known protein).
Humans have some 3,000,000,000 letters (base pairs) in their genome, so a faster approach was needed to get the project finished in the planned 15 years.
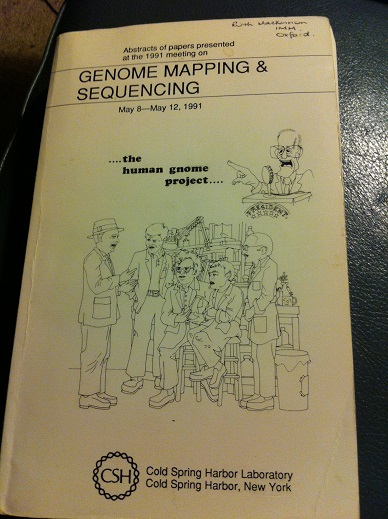
The Human Genome Project encouraged the development of much faster automated sequencing. I attended the 1991 Cold Spring Harbor Genome Mapping and Sequencing Meeting and there were several examples of exciting new automated sequencing prototypes, which used a range of different approaches.
Abstract book from the 1991 Genome Mapping and Sequencing Cold Spring Harbor meeting. Sample abstracts: “Capillary gel electrophoresis for DNA sequencing – comparison of three different approaches” (HP Swedlow et al); “Library of 256 hexamers, degenerate at two positions (5′-NNXXXX-3′), can create all possible 12-mer primers for applications in high-volulme DNA -sequencing strategies” (D.Shoemaker et al)
Now we can take it for granted that we can look up a gene on the internet. Having a human genome sequence was going to make a big contribution to health care. It is already helping, and will play a bigger role as we learn more about what roles the various genes play. For example working out what genes are playing a role in cancer will become more routine.
We can already do a lot for some cancer patients by doing genetic tests on their cancer. There are many categories of leukaemia that have a very specific type of DNA abnormality, and knowing what gene is involved can help diagnose and treat the disease appropriately.
Chromosome abnormalities helped make some of the earliest cancer gene discoveries. That’s because the gene abnormalities that cause some cancers are caused by microscopically visible changes to the chromosomes, which pinpoint the cancer gene. The poster child for this is chronic myeloid leukaemia. Most cases of CML have a chromosome abnormality known as the Philadelphia translocation. In fact this was the first cancer chromosome abnormality to be discovered. Imatinib (Glivec/Gleevec/STI-571) was one of the first targeted cancer drugs. Designed to lock onto the molecule produced by the cancer gene, it targets the leukaemia cells containing the Philadelphia chromosome. It’s made a huge improvement to the outlook for CML patients.
But for most cancers we’re not so lucky – the cancer-causing genes are not usually so obvious or easy to identify. Most cancers have their own individual combination of genetic errors, and what’s more, the genome changes as the cancer grows more aggressive and spreads. Sequencing of whole cancer genomes could become standard practice in cancer treatment, as a way of understanding each cancer and selecting treatment that targets its specific genetic changes. First we will need to be able to read a complete genome quickly and cheaply. We’re not there yet. But we’re on the way. Compared to 15 years for one representative genome, that’s impressive.
Next time: The Human Genome Project was said to be complete in 2003, in time for the 50th anniversary of the discovery of the structure of DNA. Actually it’s still not finished. Most of the gaps are regions that are very relevant to cancer.
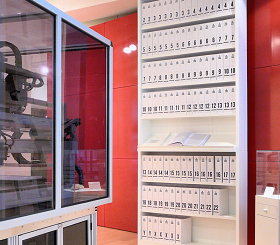
The first printout of the human genome to be presented as a series of books, displayed in the ‘Medicine Now’ room at the Wellcome Collection, London. The 3.4 billion units of DNA code are transcribed into more than a hundred volumes, each a thousand pages long, in type so small as to be barely legible. From Ross London et al en.wikipedia.
It’s getting harder to find research funding these days – it’s also a big time sink. I’m exploring different ways to raise awareness of this leukaemia research project and funds to keep it going.
Shouldn’t the government fund research? The Australian government is the largest funder of Australian medical research through the NHMRC. But there’s not enough money to fund all the worthwhile projects. Researchers spent over 500 working years making applications to just one of the NHMRC’s funding schemes last year, at a cost of $66 million (British Medical Journal report). Only one in five of the applications was funded – that’s 400 years spent writing unsuccessful grant applications, 400 years of research that was foregone to write those grants.
This project is rare in that it is addressing a very severe type of leukaemia from a different angle to the projects that are attracting large amounts of grant funding.
Have a look at the About page for more information on the project.
One consequence of funding cutbacks is that once a project is halted, the researchers move on to something else and the momentum is lost – the project is not likely to get up again and the knowledge and expertise are lost. This project is very specialised, and is supported with very little manpower (just me really) in a diagnostic laboratory.
Elizabeth Duong is a young amateur film maker based in Melbourne. With the help of some very talented friends, actors and dancers, she’s making a film to support this research project. There’s an original film score by Daniel Hernandez, to be recorded by Essendon Symphony Orchestra. They are all donating their time. The film will help raise awareness of leukaemia and leukaemia research.
With the help of our very generous donors we have raised the modest funds that we need to make the film. Thank-you to all including Caroline, Sarah, Nicholas, John and our anonymous donors.
I’ll post more information on the film as it progresses but there are good details and some photos of the first filming session through the Pozible link. Also some examples of Elizabeth’s previous work. Have a look.
This is going to be a blog about research and cancer, but I wanted to set the scene with a little insight into my workplace. Cancer can make people think about questions of life and spirituality.
Today I was talking with two people who both lost their spouses to cancer a few years ago. Both had been treated at St Vincent’s Hospital, where I work. These people commented that it’s a special hospital. The staff really care, and there’s a spiritual dimension which really made a difference.
The hospital was founded by the Sisters of Charity to serve the poor of Melbourne. It still looks out for the poor and disadvantaged, including patients of modest means. It makes an effort to reach out to the homeless, the outcasts and the mentally ill. It also provides excellent care, being a teaching hospital and part of the University of Melbourne and the Australian Catholic University, and excelling in many areas of clinical research.
One thing I like about working at St Vincent’s is “Five Minutes on Friday” – a weekly inspirational message from the Director of Mission. I thought I should share part of this week’s timely offering from Lisa McDonald.
“One of the curious quirks of having a job with the word ‘Mission’ in the title is that it is not unusual for people to expect you would have such things as:
1. A reasonable knowledge of Catholic heritage
2. The capacity to quote a scripture or two… or three
3. The phone number of the Sister’s convent on speed dial
and, here’s a curious one… a favourite Church season!
Highly convenient of me to have mentioned it because (aside from Christmas obviously), we’re about to start mine. Pentecost…. “
Which is a weekly reminder that the people we are trying to help, whether they have a faith or not, are more than just flesh and blood.









{kind=link}