When it was initiated by the US Department of Energy in 1987, the Human Genome Project was an ambitious, some said impossible, endeavour. It was all about producing a representative readout of the human genome – that is, the whole set of human DNA.
At the time DNA was read (sequenced) manually – scientists read each letter of the code off an X-ray film. One by one genes were laboriously found and sequenced. Finding and characterising a gene in this way was a whole PhD project, if you got lucky and actually found the gene (finding a gene by family studies was harder than starting with a known protein).
Humans have some 3,000,000,000 letters (base pairs) in their genome, so a faster approach was needed to get the project finished in the planned 15 years.
The Human Genome Project encouraged the development of much faster automated sequencing. I attended the 1991 Cold Spring Harbor Genome Mapping and Sequencing Meeting and there were several examples of exciting new automated sequencing prototypes, which used a range of different approaches.
Abstract book from the 1991 Genome Mapping and Sequencing Cold Spring Harbor meeting.
Sample abstracts: “Capillary gel electrophoresis for DNA sequencing – comparison of three different approaches” (HP Swedlow et al); “Library of 256 hexamers, degenerate at two positions (5′-NNXXXX-3′), can create all possible 12-mer primers for applications in high-volulme DNA -sequencing strategies” (D.Shoemaker et al)
Now we can take it for granted that we can look up a gene on the internet. Having a human genome sequence was going to make a big contribution to health care. It is already helping, and will play a bigger role as we learn more about what roles the various genes play. For example working out what genes are playing a role in cancer will become more routine.
We can already do a lot for some cancer patients by doing genetic tests on their cancer. There are many categories of leukaemia that have a very specific type of DNA abnormality, and knowing what gene is involved can help diagnose and treat the disease appropriately.
Chromosome abnormalities helped make some of the earliest cancer gene discoveries. That’s because the gene abnormalities that cause some cancers are caused by microscopically visible changes to the chromosomes, which pinpoint the cancer gene. The poster child for this is chronic myeloid leukaemia. Most cases of CML have a chromosome abnormality known as the Philadelphia translocation. In fact this was the first cancer chromosome abnormality to be discovered. Imatinib (Glivec/Gleevec/STI-571) was one of the first targeted cancer drugs. Designed to lock onto the molecule produced by the cancer gene, it targets the leukaemia cells containing the Philadelphia chromosome. It’s made a huge improvement to the outlook for CML patients.
But for most cancers we’re not so lucky – the cancer-causing genes are not usually so obvious or easy to identify. Most cancers have their own individual combination of genetic errors, and what’s more, the genome changes as the cancer grows more aggressive and spreads. Sequencing of whole cancer genomes could become standard practice in cancer treatment, as a way of understanding each cancer and selecting treatment that targets its specific genetic changes. First we will need to be able to read a complete genome quickly and cheaply. We’re not there yet. But we’re on the way. Compared to 15 years for one representative genome, that’s impressive.
Next time: The Human Genome Project was said to be complete in 2003, in time for the 50th anniversary of the discovery of the structure of DNA. Actually it’s still not finished. Most of the gaps are regions that are very relevant to cancer.
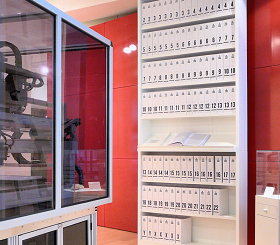
The first printout of the human genome to be presented as a series of books, displayed in the ‘Medicine Now’ room at the Wellcome Collection, London. The 3.4 billion units of DNA code are transcribed into more than a hundred volumes, each a thousand pages long, in type so small as to be barely legible. From Ross London et al en.wikipedia.

Great post Ruth! What did you present at that ’91 meeting? I love the whimsy of printing the entire genome in a series of books. So mind-boggling to think that all that information is printed several trillion times over in each human body.
Yes, mind-boggling indeed, and to think of the speed at which it’s happening. In 1991 I was doing my postdoc in Kaye Davies’ lab at Oxford hunting down the fragile X gene. I presented work on a clone from a microdissection library from the fragile X region, from Uwe Claussen and Bernhard Horstemke, pioneers of microdissection. The clone turned out to be in the nearby L1CAM gene but was very interesting. I also co-authored Andre Rosenthal’s poster – he used the clone as a starting point for his PCR walking technique. At the Cold Spring Harbor meeting Agi Gedeon from Grant Sutherland’s lab (where I did my PhD) announced that they’d cloned (beaten us to) the fragile X gene. The back of the abstract book is even better – more gnomes – it doesn’t scan well because it’s drawn with very fine lines but I’ll try and get it into my next post.
Ouch. Being beaten to the punch can’t feel good!
[…] https://chromosomesandcancer.com/2013/06/18/the-human-genome-project-and-cancer/ […]